
Authors
Benjamin Ryan, PhD MPH REHS, FRRHHed1; Deon Canyon, PhD, DBA, MPH, FACTM2; Raelene Lockhorst, GAICD, MA, GradDipIntRel, GradCertDefStud 3; Len Notaras AO, Bmed, LLB, BA (Hons), Dip Com, MHA4
- Professor, Frist College of Medicine, Belmont University, Nashville, TN, USA
- Associate Dean, Daniel K. Inouye Asia-Pacific Center for Security Studies, Honolulu, HI, USA
- Deputy Director National Security Program, Australian Strategic Policy Institute, Canberra, ACT, Australia
- Executive Director, National Critical Care and Trauma Response Centre, Darwin, NT, Australia, Professor Fellow Flinders University of South Australia
Abstract
The U.S., Australia, and the Indo-Pacific are facing its most challenging strategic environment since the Second World War. A ten-year window of warning for a conflict no longer exists. The urgency of ramping up readiness is demonstrated by U.S. military leaders predicting the People’s Republic of China (PRC) will be ready to invade Taiwan in 2027. In this scenario, the U.S. wounded could range from 9,500 to 100,000 troops in the first 100 days, higher than more than 20 years of war in Afghanistan and Iraq. Diplomatic fragility of the region could compromise access, basing, and overflight, making Australia the only reliable sovereign allied territory in the region. As a result, wounded personnel would face 10-to-14-hour evacuation timelines from the war zone to Darwin (far exceeding the “golden hour” standard). To maximize readiness and minimize casualties in this scenario, Australia and U.S. must urgently establish civil-military medical-focused agreements, planning, and exercises for Northern Australia. Translating this into action would require specific lines of effort to complement the Australian and U.S. defense posture in Northern Australia. These include strategies for mitigating diplomatic fragility, increased health system capacity in Northern Australia, integrated civil-military readiness, preparedness for chemical, biological, radiation, nuclear and explosive (CBRNE) emergencies, and health tech innovation. Northern Australia now represents an essential component of a distributed medical network for the U.S. and allies by providing strategic depth that Guam cannot offer due to its vulnerability to PRC strikes.
Introduction
Northern Australia holds critical geopolitical importance for deterrence and defense posture in the Indo-Pacific, with a growing military presence from both Australian and U.S. forces. The region is facing its most challenging strategic environment since the Second World War and a ten-year window of warning for a conflict no longer exists.1 The urgency of ramping up readiness is demonstrated by U.S. military leaders predicting the People’s Republic of China (PRC) will be ready to invade Taiwan in 2027.2,3 In this scenario, the U.S. wounded could range from 9,500 to 100,000 troops in the first 100 days, higher than more than 20 years of war in Afghanistan and Iraq.3 This number of wounded would be a catastrophic mismatch with the current U.S. medical capacity in the region. For example, the U.S. Naval Hospital Okinawa, Japan, has 79 beds, U.S. Naval Hospital Yokosuka, Japan, 47 beds, Brian D. Allgood Army Community Hospital, Pyeongtaek, South Korea, 68 inpatient beds and the U.S. Naval Hospital Guam 39 to 42 beds. The U.S. Naval Hospital Okinawa is the largest medical asset in the first island chain, and requires “significant buttressing” to reach a Role 3 standard (advanced diagnostics and surgery).4 Currently, the largest military treatment facility in the Pacific Rim is Tripler Army Medical Center in Hawaii with 450 beds, which is roughly 5,000 miles from the first island chain.5 Diplomatic fragility could also impact access, basing, and overflight routes for medical evacuations, which makes Northern Australia the closest reliable sovereign allied territory in the region.
Due to the geographic vulnerability of Guam to PRC strikes, Northern Australia represents an opportunity to bolster the distributed medical network in the Indo-Pacific. This region is vital due to the proximity of key maritime trade routes and regional partners, positioning it as a crucial node for deterrence and engagement with allies and partners in the Indo-Pacific.6 A historical example of this significance was the bombing of Darwin during the Second World War on February 19, 1942, when 188 carrier-based Japanese bombers dropped more, but smaller, bombs than on Pearl Harbor to disrupt allied shipping, damage morale, and prevent this location from being used as a springboard for counter-attacks across the region.7,8 Northern Australia encompasses the Northern Territory and parts of Queensland and Western Australia that intersect with the Tropic of Capricorn, and is home to a range of military including joint Australia-U.S. facilities, critical fuel storage, and reserve infrastructure (Figure 1).9
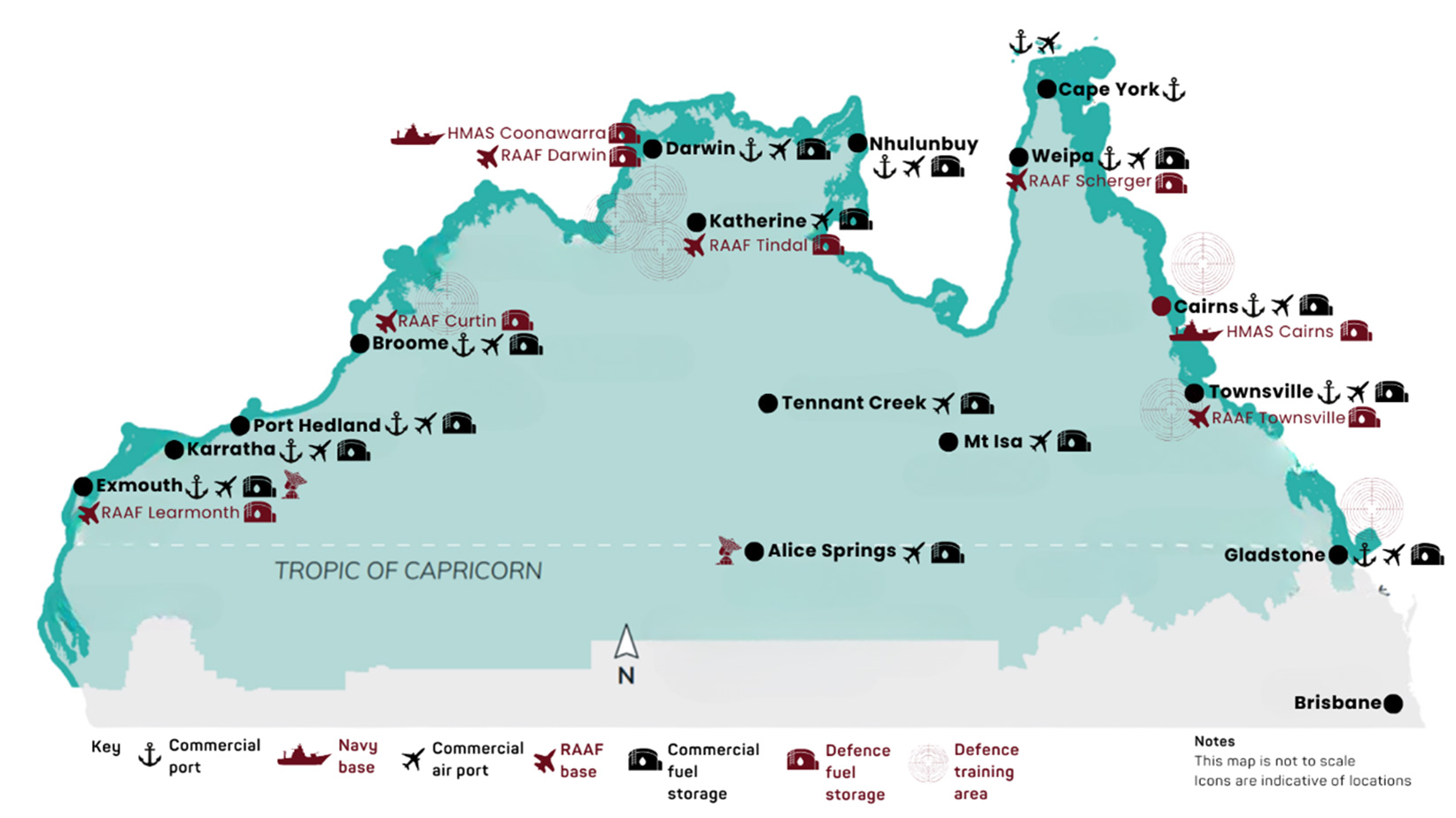
Figure 1 – Northern Australia Military Bases6
The Australian Government’s 2024 National Defence Strategy has reinforced the importance of building resilience in Northern Australia as a foundation for Indo-Pacific regional security.1 The U.S. 2026 National Defense Strategy also highlights the need for deterrence in the Indo-Pacific and to prevent domination by any single competitor nation.10 The significance of Northern Australia has been recognized by the United States Security of War Pete Hegseth who stated on December 8, 2025, “We’re upgrading the infrastructure on airbases in Queensland and the Northern Territory…so more U.S. Marines can do rotational deployments and pre-positioning MV-22 Ospreys”.11 These efforts underscore the enduring need for a well-prepared and well-defended Northern Australia to offer strategic deterrence and force posture in the Indo-Pacific.12
A PRC attack could begin with multi-domain strikes against key Taiwan military forces along with U.S. bases in the region and naval forces inside the second island chain to make it difficult for international partners to rapidly intervene.13 Simultaneously, the PRC could use cyber, electronic, and information operations to degrade the U.S. and allied intelligence and disorientate response forces.13,14 Northern Australia is far enough away to avoid having the large volume of missile fires that could confront Taiwan, Japan, and other forces but is close enough to be operationally relevant and a stronghold.15 In such a scenario, Northern Australia, especially Darwin and Katherine, could serve as a resilience cornerstone for allied operations and support.13
Fundamental for resilience and force posture in the region is strengthening Australia-U.S. cooperation. This includes driving interoperability and interchangeability through increasing collaboration on defense innovation, science and technology.1 In recognition of this the U.S. Department of War has elevated the Defense Industrial Base (DIB) to a national security priority with the emphasis on production and innovation expanded to shaping alliances, deterrence, and influence.16 An example of this pivot is the enhanced U.S. and Australia partnership to rapidly manufacture hardware and supplies for militaries, including aircraft, ships, submarines, missiles, bombs, ammunition, firearms and combat vehicles.11 In Australia, deterrence encompasses expanding the DIB while also remaining the partner of choice in the region, having resilient bases in Northern Australia, and adopting civil-military arrangements in a crisis.1 Readiness and resilience efforts in Northern Australia and across the Indo-Pacific must recognize that a crisis or conflict in the Taiwan Strait could rapidly reshape the region’s security environment.
Despite this threat, disaster management and health systems in Australia continue to be primarily focused on extreme weather events.17,18 This leaves a large gap in civil-military readiness for combat and conflict-related threats in Northern Australia and the surrounding region. This is despite the bombing of Darwin in 1942 resulting in more deaths than Cyclone Tracy in 1974 and decades of infrastructure design and upgrades intended to better withstand extreme weather events.19 To address these gaps and prepare for the possibility of conflict, a targeted civil-military focus on health security and resilience is required. Health security refers to measures and activities taken to protect people’s health against threats or harmful events.20 This often encompasses the threat of influenza and other respiratory diseases, novel diseases, bioterrorism, and disasters.20-22
To rapidly strengthen health security and resilience in Northern Australia, the logical starting point would be to bolster U.S. investment and engagement in Darwin through the National Critical Care and Trauma Response Center (NCCTRC). This is an Australian Government asset, funded primarily by the Department of Health, Disability and Ageing, and also by the Department of Foreign Affairs and Trade, with significant programs in the Indo-Pacific.The NCCTRC coordinates the rapidly deployable Australian Medical Assistance Team (AUSMAT). This capability was established following Darwin’s response to the 2002 Bali bombings. It has become a central component of the Australian Government’s disaster and emergency medical preparedness and response capability.23 NCCTRC has experience in civilian-military cooperation with the U.S. and allies, demonstrated in August 2023, when the service provided critical care through the Royal Darwin Hospital to U.S. Marines following the MV-22B Osprey crash during Exercise Predators Run in August 2023.24 The rapid integration of Australian civilian medical infrastructure with U.S. military evacuation and treatment systems provided a real-world test of interoperability, underscoring Darwin’s ability to surge to support role as a forward medical stabilization hub for allied operations in Northern Australia.
Translating this into action would require specific lines of effort to complement the defense posture in Northern Australia. These include mitigating the impact of diplomatic fragility, integrated civil-military preparedness, increased health system capacity, preparedness for chemical, biological, radiation, nuclear and explosive (CBRNE) emergencies, and health tech innovation. By addressing these risks through an Australian and U.S., collaboration, a framework would be set to strengthen resilience in Northern Australia and the Indo-Pacific. A pathway for achieving this is provided in Figure 2 and described in the following. Delivering on this would also align with the intent of the U.S. National Defense Authorization Act for Fiscal Year 2026, particularly in the areas of emerging technologies, deterrence, and defense posture in the Indo-Pacific.25
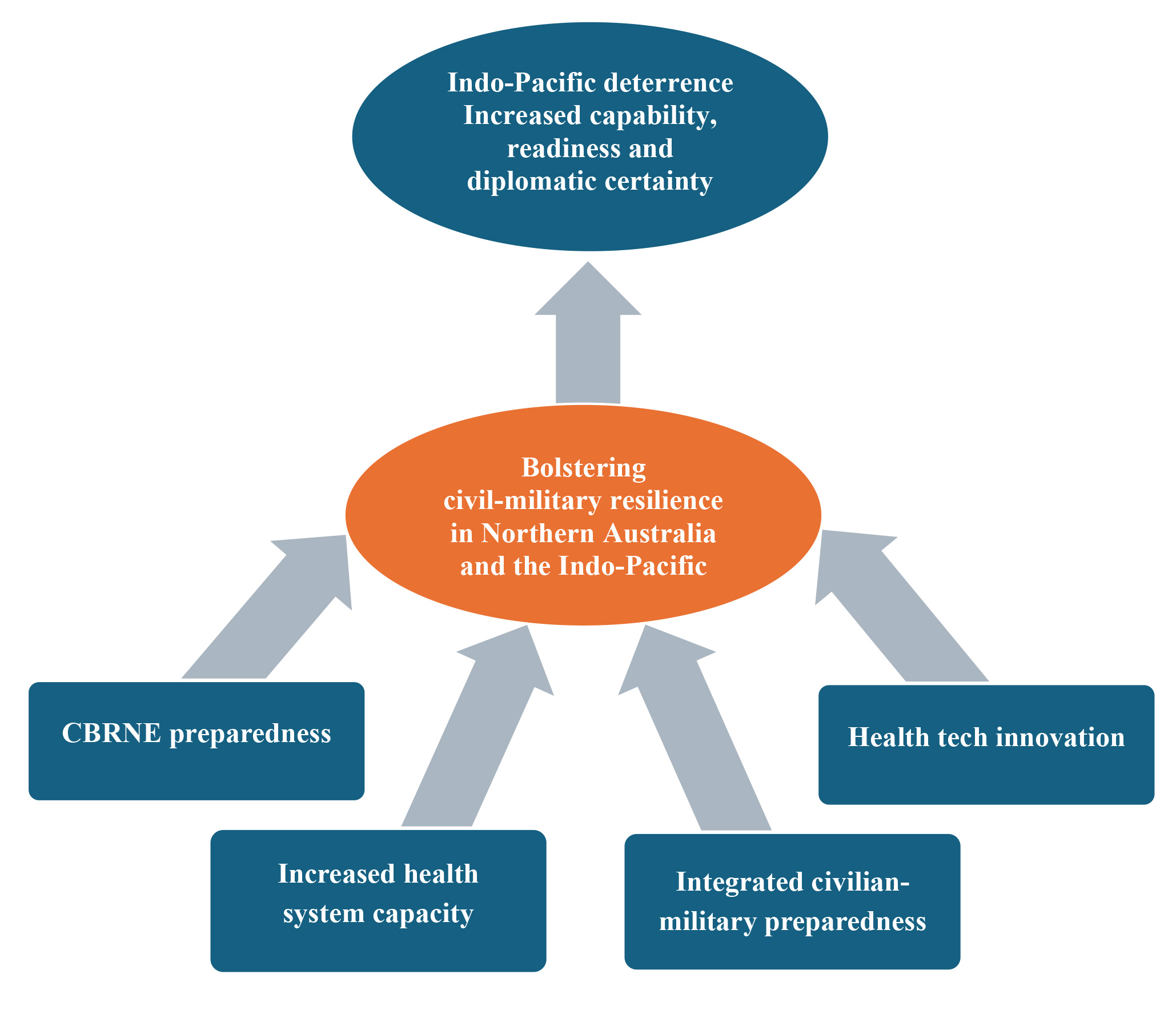
Figure 2 – Framework for Detering Adversary Power: Bolstering Civil-Military Resilience in Northern Australia
Strategic fragility for access, basing and overflight
Access, basing, and overflight (ABO) arrangements are foundational to U.S. power projection in the Indo-Pacific, but they cannot be assumed in a conflict scenario. U.S. force projection relies on overseas bases and military access arrangements across nations that practice strategic hedging rather than outright alignment with either Washington or Beijing. The diplomatic landscape across Southeast Asia presents the most acute ABO risk. Indonesia is the guardian of critical maritime choke points including the Sunda and Malacca Straits. It adheres to a “bebas-aktif” non-aligned foreign policy. A 2025 Center for Strategic & International Studies (CSIS) analysis modelled a scenario in which a U.S. carrier strike group ordered to the South China Sea during a Taiwan crisis is denied transit through Indonesian waters and airspace, resulting in a costly strategic detour through the Timor and Arafura Seas.26 Indonesia is not unique in this posture. The ISEAS–Yusof Ishak Institute’s 2024 State of Southeast Asia Survey found that approximately half of the countries would align with Beijing if forced to choose, revealing deep economic reliance on the PRC.27 For medical evacuation in particular, this creates a risk that overflight permissions could be denied or delayed, precisely when speed is most critical to casualty survival.
ABO fragility is compounded by the vulnerability of Guam. The People’s Liberation Army (PLA) Rocket Force reportedly holds an arsenal of more than 400 missiles capable of reaching the island, and the CSIS Taiwan wargame found that PRC attacks on Andersen Air Force Base occurred in all 24 modelled scenarios.28 A hub struck in the opening hours of conflict cannot simultaneously function as a secure medical evacuation node, revealing a foreseeable break in casualty care chains.
Northern Australia is not immune to long-range strike, but it’s geography would require a disproportionate effort to generate sustained effects. This relative sanctuary, combined with proximity to Indo-Pacific operating areas, makes it a resilient rear-area hub rather than a frontline target. As a sovereign allied state, it does not carry the diplomatic conditionality risks characterizing Southeast Asian ABO arrangements. Despite this strategic advantage, the U.S. and Australia have not formalized civil-military medical agreements for operationalizing Northern Australia as a designated evacuation and treatment hub. Existing alliance instruments, such as the Australia-U.S. Force Posture Initiative (USFPI) address force posture and logistics but do not specify medical evacuation routing, hospital surge agreements, or pre-positioning protocols.11 This gap means the most reliable ABO territory in the region would not be ready to receive mass casualties when it matters most.
Two political dimensions also require resolution: Australian public acceptance of large numbers of U.S. combat casualties transiting through Darwin, and the PRC’s likely response to Northern Australia explicitly functioning as a medical hub. Beijing would certainly frame this role as direct involvement in hostilities. Addressing this ABO fragility requires bilaterally agreed medical evacuation routing embedded in formal instruments, civil-military training and exercises rehearsing mass casualty reception at Darwin and NCCTRC, and early strategic communications engagement with both Australian domestic audiences and regional partners.
Integrated civil-military preparedness
The evolving geopolitical dynamics in the Indo-Pacific, underscores the urgent need for robust preparedness, especially in healthcare, to support communities in Northern Australia and strengthen military readiness.1 The Australian Civil-Military Centre’s report, Considerations for Civil-Military Interaction During Public Health Emergencies, highlights the importance of integrated planning, augmentation of the workforce, and capacity building through global engagement to address public health risks.29 According to the report Building national preparedness: A road map for Australia and what we should learn from Finland, Australia lacks an effective interagency collaboration system involving the military, police, emergency services, healthcare, and intelligence agencies.30 Imperative to addressing this would be a shift towards established and practiced networks across disciplines, industry, and the civilian and military sectors.31
To address this gap, there is an urgent need to better understand vulnerabilities and capacity constraints of Northern Australia’s health system. Darwin faces distinct challenges, including geographic isolation, workforce shortages, and limited infrastructure. These are constraints that would be further strained by increased military activity.32 Ensuring civilian and military communities in this region have access to adequate healthcare is fundamental to sustaining operations and war fighter readiness. This necessitates a comprehensive civil-military assessment by Australian and U.S. partners to create a locally informed action plan for both countries to rapidly strengthen health system integration, coordination, and resilience in Northern Australia.
Increased health system capacity
Northern Australia represents an essential component of a distributed medical network, providing strategic depth that Guam cannot offer due to its vulnerability to PRC strikes. There is a catastrophic mismatch between projected casualties (9,500-100,000) and U.S. medical capacity in the Indo-Pacific with fewer than 300 hospital beds in total (excluding, Tripler Army Medical Center in Hawaii). If fragile ABO agreements fail, this could sever evacuation routes to facilities in Japan, South Korea, and even Hawaii.
Despite their substantial capacity, the availability of U.S. hospital ships cannot be assumed. Both USNS Mercy and USNS Comfort were reported in early 2026 to be simultaneously undergoing maintenance in dry dock in Mobile, Alabama.33 This highlights a structural constraint in relying on these vessels for rapid response: they require activation time, lengthy transits, and permissive operating conditions before functioning as theatre medical hubs. In a Taiwan conflict scenario, where peak casualties would likely occur in the opening weeks, hospital ships represent strategic depth rather than immediate medical support, reinforcing the importance of resilient land-based civil–military health infrastructure. The NCCTRC partially addresses this gap. NCCTRC’s response to the 2023 MV-22B Osprey crash demonstrated its capacity to receive and treat U.S. combat casualties under real conditions, with critically injured Marines stabilized and managed through the Royal Darwin Hospital before onward transfer.24 However, NCCTRC’s current configuration is designed for disaster response and trauma management, not sustained mass casualty operations at wartime scale.
Concrete investment in training, systems, and infrastructure is required. This is because NCCTRC relies on Royal Darwin Hospital infrastructure/beds. For this reason, an expansion of Royal Darwin Hospital’s inpatient capacity up to 200-bed surge capability would begin to close the gap between projected casualties and available treatment beds within an allied sovereign state. Pre-positioned forward surgical teams and the establishment of the first allied blood bank outside U.S. territory in Darwin would help address the two most time-critical constraints in combat casualty care: surgical intervention and blood resuscitation.4 Additionally, there would need to be investments in radiology capacity and training/accreditation of U.S. personnel to work in this type of surge. These investments would also serve non-conflict purposes, strengthening Northern Australia’s capacity to respond to the large-scale natural disasters and pandemics that regularly stress the region’s health systems, generating dual use returns on alliance investment.
CBRNE preparedness
There is limited CBRNE awareness, deployment experience, and capabilities in Northern Australia. More broadly, Australia remains insufficiently prepared to respond to a CBRNE attack on, or in, its strategic area of interest.34 Risk exposure is increasing as nuclear-powered submarine operations expand, civil nuclear energy adoption accelerates across the Indo-Pacific, regional CBRNE weapon capabilities advance, and geopolitical tensions intensify.35-37 The need to strengthen military preparedness was demonstrated in mid-2025 when U.S. and Australian forces conducted a joint exercise focused on enhancing CBRNE defense capabilities.38 However, civilian medical staff and emergency management personnel often lack the training and confidence required for a response to nuclear or radiologic incidents.39 Also, there is generally a reluctance to respond compared to other potentially hazardous events.40 In a conflict or crisis scenario, this could delay casualty treatment, complicating evacuation operations, and significantly degrade recovery outcomes.
To address this risk there is an urgent need to identify, rank, and prioritize strategies to advance CBRNE preparedness across northern Australia. One suitable approach would be the application of a “Scorecard” methodology, which has proven effective in civilian settings globally.40-48 This has included the development of a pilot scorecard focused on nuclear and radiation preparedness, applied in Montgomery, Alabama, in mid-2024, and a chemical and waste version tested in Wellington, New Zealand, in October 2024. Funders for this method have included the U.S. Department of Agriculture49 and the Japan Science and Technology Agency45. The Scorecard approach is versatile and scalable, designed to inform decision making and build capacity by systematically leveraging local insights to inform development and implementation of local to regionally informed action plans. This process would produce feasible, targeted strategies to strengthen CBRNE preparedness across Northern Australia.
Health tech innovation
Rising geopolitical tensions have driven a dramatic increase in global military expenditure, a trend expected to continue.50 This shift is reshaping public and private investment priorities toward technologies with defense relevance. Governments and investors are increasingly elevating dual‑use domains, including biotechnology and artificial intelligence, within defense strategies and innovation programs.51 Across the U.S., European Union, and NATO, this trend is accelerating the integration of commercially developed technologies into security ecosystems. While this trajectory strengthens deterrence and readiness, it risks overlooking civil-military health resilience, especially in austere and remote environments such as Northern Australia and other parts of the Indo-Pacific.
To address this challenge, Australia and the U.S. should create a process to assess early-stage health technologies for their applicability in civilian, austere, and deployment settings. This would be directly aligned with DIB priorities. In the Australian context, NCCTRC’s Bees Creek Training Facility would be an ideal setting. This facility is designed to prepare Australian and international health personnel for emergency responses. The facility can be designed to reflect an austere environment where both civilians and military personnel can work in partnership to assess early-stage health technologies for their applicability in humanitarian, austere, and deployment settings.
By combining expert consensus with a structured evaluation criterion, this process could generate the evidence based needed for funders, investors, and policymakers to identify health technology innovations capable of meeting both civilian health and defense needs. This type of civil-military and Australian-U.S. partnership could leverage shared simulation capabilities and clinical expertise to influence health technology development across Northern Australia and the broader Indo-Pacific. Ultimately, providing the framework needed for ensuring dual-use innovation remains aligned with bolstering deterrence and war fighting capability across the Indo-Pacific. Establishing such a framework would help to ensure dual use innovation contributes not only to technological advancement, but also to operational resilience, sustained medical support and overall deterrence effectiveness.
Where current domestic fiscal constraints limit the Australian federal government or Northern Territory government contributions, this framework could be advanced through United States Force Posture Initiatives (USFPI)52 funding and blended public-private investment. U.S. support could be delivered under the Pacific Deterrence Initiative, which focuses on countering China’s military assertiveness in the Indo-Pacific.53 In this situation, investment could be directed toward deployable medical capability, interoperability training and technology validation. Complementary private-sector participation could be enabled through a public-private partnership centered on the NCCTRC, positioning Northern Australia as a dual-use health technology testing and validation environment. By aligning commercial innovation incentives with allied operational requirements, this approach would reduce reliance on constrained public budgets while accelerating capability development that strengthens deterrence, force protection and regional resilience.
Conclusion
Northern Australia represents an essential component of a distributed medical network for the U.S. and allies by providing strategic depth that Guam cannot offer. This is the only reliable sovereign allied state in the region, however, the U.S. and Australia lack medical-focused agreements, planning, and exercises. The catastrophic mismatch between projected casualties (9,500-100,000) and U.S. medical capacity in the Indo-Pacific highlights the urgent need to bolster civil-military resilience in Northern Australia. Implementation of the proposed framework would build on existing efforts to address an existing gap in strategic deterrence and resilience for Northern Australia and the Indo-Pacific. Addressing strategic fragility would also mitigate the risk of access, basing, and overflight being compromised during a conflict scenario. Increasing the health system capacity through additional hospital beds, pre-positioned surgical and medical teams, and establishment of a blood bank would maximize readiness and response capacities for conflict and non-conflict emergencies among allies and partners.
Integration of civil-military preparedness, especially for the health system in Northern Australia, would improve healthcare access for civilians and war fighters alike. CBRNE capabilities remain limited in Northern Australia, posing a growing risk to allied resilience in the Indo-Pacific. By advancing CBRNE preparedness, Northern Australia could rapidly evolve into a deployment hub and regional treatment center during a conflict or crisis, as demonstrated during the 2002 Bali bombings response. Creation of civil-military health technology innovation across at NCCTRC in collaboration with U.S. partners would be directly aligned with DIB priorities and further strengthen innovation gains across allies and partners. Delivering on this framework would also help achieve the goals of the U.S. National Defense Authorization Act for Fiscal Year 2026, National Security Strategy of the United States of America, and the Australian Government’s National Defence Strategy. Ultimately, this approach offers a practical pathway for Australia and the U.S. to strengthen strategic deterrence through resilience and an integrated civil-military defense posture in the Indo-Pacific.
References
- Australian Government. National Defence Strategy 2024. https://www.defence.gov.au/about/strategic-planning/2024-national-defence-strategy-2024-integrated-investment-program
- Cancian M, Cancian M, Heginbotham E. The First Battle of the Next War: Wargaming a Chinese Invasion of Taiwan. Center for Strategic and International Studies. Accessed December 10, 2025. https://www.csis.org/analysis/first-battle-next-war-wargaming-chinese-invasion-taiwan
- Goralnick E, Holcomb JB, Elster EA. Preparing the Civilian Health Care System for Wartime: A National Imperative for Military-Civilian Integration. JAMA. 2025;334(19):1703–1704. doi:10.1001/jama.2025.18642
- Lin A, Arfsten D, Cole J, Hghey S, Kotler J. Expeditionary Advanced Medical Care for the Indo-Pacific. Proceedings 2025;151/4/1,466
- Economy HD. Tripler Army Medical Center. Accessed February 20, 2026. https://defenseeconomy.hawaii.gov/tripler-army-medical-center/
- Lockhorst R. The Critical Role of Northern Australia in Australian and Indo-Pac Defence. DEFENSE.info. Accessed December 12, 2025. https://defense.info/partners-corner/2025/04/the-critical-role-of-northern-australia-in-australian-and-indo-pac-defence/
- Berra T. The Bombing of Darwin Remembered. U.S. Naval Institute Accessed December 10, 2025. https://www.usni.org/magazines/naval-history-magazine/2022/april/bombing-darwin-remembered
- Australia NAo. The bombing of Darwin. National Archives of Australia. Accessed December 12, 2025. https://www.naa.gov.au/help-your-research/fact-sheets/bombing-darwin#:~:text=Contrary%20to%20widespread%20belief%20at,would%20help%20achieve%20that%20aim
- Australian Government. Office of Northern Australia. Accessed December 18, 2025. https://www.infrastructure.gov.au/territories-regions/regional-australia/office-northern-australia
- 2026 National Defense Strategy (2026).
- Topez C. U.S., Australian Cooperation on Land, Air, Sea, Industrial Base Top Topics at 40th AUSMIN. U.S. Department of War Accessed October 12, 2025. https://www.war.gov/News/News-Stories/Article/Article/4354644/us-australian-cooperation-on-land-air-sea-industrial-base-top-topics-at-40th-au/
- Bickerton M. Darwin bombing a call to defend the north. Australian Government – Defence Accessed December 10, 2025. https://www.defence.gov.au/news-events/news/2025-02-28/darwin-bombing-call-defend-north
- Pettyjohn S. More than the Sum of its Parts: Developing a Coordinated US-Australian Response to Potential Chinese Aggression. 2024;
- Wuthnow J, Grossman D, Saunders PC, et al. Crossing the Strait: China’s military prepares for war with Taiwan. National Defense University Press; 2022.
- Mahnken T. INDO-PACIFIC STRONGHOLD NORTHERN AUSTRALIA’S ROLE IN THE AUSTRALIA-U.S. ALLIANCE. 2025. https://csbaonline.org/uploads/documents/CSBA8406_(Indo-Pacific_Stronghold_Report)_Final_web.pdf
- Canyon DV. Adaptive Power Helps the U.S. Defense Industrial Base Become a Tool of Deterrence. Security Nexus 2025;
- Nanthini S. A climate security priority: Australia’s need for balanced domestic disaster infrastructure. S. Rajaratnam School of International Studies https://www.rsis.edu.sg/wp-content/uploads/2024/02/IP24013.pdf
- Australian Government. Alternative Commonwealth Capabilities for Crisis Response. 2023. https://www.homeaffairs.gov.au/reports-and-pubs/files/alternative-clth-capabilities-crisis-response.pdf
- LOCKHORST R, COYNE J. Cyclone Tracy: 50 years on. 2024;
- Mauer N, Scarpetti G, Wismar M. A public debate on the future health priorities of the European Union: Outcomes, insights and ideas for action. Copenhagen: WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies. 2024;
- Office of Global Affairs. Global Health Security U.S. Departmetn of Health and Human Services Accessed December 10, 2025. https://www.hhs.gov/about/agencies/oga/global-health-security/index.html
- CDC. Global Health Security. U.S. Centers for Disease Control and Prevention Accessed December 10, 2025. https://www.cdc.gov/global-health/topics-programs/global-health-security.html
- NCCTRC. About NCCTRC. National Critical Care and Trauma Response Center Accessed December 12, 2025.
- Commonwealth of Australia. National trauma centre ready for future health crisis. Commonwealth of Australia. Accessed December 12, 2025. https://www.health.gov.au/ministers/the-hon-mark-butler-mp/media/national-trauma-centre-ready-for-future-health-crisis#:~:text=As%20well%20as%20international%20events,Australia%20once%20they%20were%20stabilised
- 119th Congress. S.2296 – National Defense Authorization Act for Fiscal Year 2026. 2025.
- Panjeti P. Navigating the Divide: Why the U.S. Navy Must Resume FONOPs in Indonesia. Center for Strategic & International Studies Accessed February 20, 2026. https://www.csis.org/analysis/navigating-divide-why-us-navy-must-resume-fonops-indonesia
- Seah S, Lin J, Martinus M, et al. The State of Southeast Asia: 2024 Survey Report. Vol. 2026. 2024. https://www.iseas.edu.sg/wp-content/uploads/2024/03/The-State-of-SEA-2024.pdf
- Guam: Defense Infrastructure and Readiness – R47643 (Congressional Research Service) (2023).
- ACMC. Considerations for Civil-Military Interaction During Public Health Emergencies Australian Government. Accessed December 10, 2025. https://www.acmc.gov.au/sites/default/files/2024-09/Health%20Publication%20No5%20Electronic%20Final.pdf
- Ablong M. Building national preparedness: A road map for Australia and what we should learn from Finland. Australian Strategic Policy Institute https://aspi.s3.ap-southeast-2.amazonaws.com/wp-content/uploads/2025/05/22135215/Building-national-preparedness-1.pdf
- Farhat H, Alinier G, Chaabna K, et al. Preparedness and emergency response strategies for chemical, biological, radiological and nuclear emergencies in disaster management: a qualitative systematic review. Journal of Contingencies and Crisis Management. 2024;32(3):e12592.
- Northern Territory PHN. Urgent action needed to sustain NT’s primary healthcare workforce. Northern Territory PHN,. Accessed December 10, 2025. https://ntphn.org.au/news/2025-health-workforce-needs-assessment-report-key-challenges-and-response-plans
- Schuler M. Trump Announces Greenland Hospital Ship Mission as Mercy and Comfort Sit in Alabama Shipyard. qCaptain. Accessed March 2, 2026. https://gcaptain.com/trump-announces-greenland-hospital-ship-mission-as-mercy-and-comfort-sit-in-alabama-shipyard/
- van Ash E. Australian CBRN Health Systems Preparedness and Governance. Charles Darwin University Australia Accessed December 18, 2025. https://www.cdu.edu.au/northern-institute/engage/northern-institute-events/australian-cbrn-health-systems-preparedness-governance
- Regal Intellgence. The Growing Role of Nuclear Medicine in Modern Healthcare. Pharmiweb.com Accessed December 10, 2025.
- Rapier R. Global Nuclear Power Hits Record High as Asia Surges Ahead. OILPRICE.COM. Accessed December 10, 2025. https://oilprice.com/Alternative-Energy/Nuclear-Power/Global-Nuclear-Power-Hits-Record-High-as-Asia-Surges-Ahead.html
- Rafiq A. Resurgence Of Geopolitical Tensions In Indo-Pacific: Implications For Global Stability – OpEd. Eurasia Review. Accessed December 10, 2025. https://www.eurasiareview.com/22082024-resurgence-of-geopolitical-tensions-in-indo-pacific-implications-for-global-stability-oped/
- U.S. Department of War. U.S., Australia Conduct Joint Chemical, Biological Exercise. Accessed December 18, 2025. https://www.war.gov/News/News-Stories/Article/Article/4290094/us-australia-conduct-joint-chemical-biological-exercise/
- Dallas CE, Klein KR, Lehman T, Kodama T, Harris CA, Swienton RE. Readiness for radiological and nuclear events among emergency medical personnel. Frontiers in public health. 2017;5:202.
- Gale RP, Armitage JO. Are we prepared for nuclear terrorism? New England Journal of Medicine. 2018;378(13):1246–1254.
- Disaster Resilience Scorecard for Cities – Public Health System Resilience Addendum. https://mcr2030.undrr.org/public-health-system-resilience-scorecard.
- Jones K, Pascale F, Wanigarathna N, Morga M, Sargin S. Critical evaluation of the customisation process of the UNDRR disaster resilience scorecard for cities to earthquake-induced soil liquefaction disaster events. Bulletin of Earthquake Engineering. 2021;19(10):4115–4143.
- UNDRR. Disaster Resilience Scorecard for Cities: Food System Resilience – Addendum Accessed March 25, 2022. https://mcr2030.undrr.org/food-system-resilience-scorecard
- Tayfur İ, Şimsek P, Gunduz A, Kako M, Nomura S, Ryan B. Strengthening Public Health System Resilience to Disasters in Türkiye: Insights from a Scorecard Methodology. Disaster Prevention and Management Journal Under Review;
- Kako M. Resilience of public health systems towards “building back better”: Evaluation analysis using scorecards. Accessed December 19, 2024. https://app.dimensions.ai/details/grant/grant.13822944
- Tayfur I, Şimşek P, Gunduz A, Kako M, Nomura S, Ryan B. Strengthening public health system resilience to disasters in Türkiye: Insights from a scorecard methodology. International Journal of Disaster Risk Reduction. 2024/10/15/ 2024;113:104869. doi:https://doi.org/10.1016/j.ijdrr.2024.104869
- Williams P. Using the Results of the Public Health Scorecard Addendum in Local Resilience Planning. Online Training – Resilience of Local Governments: A Multi-Sectoral Approach to Integrate Public Health and Disaster Risk Management. United Nations Office for Disaster Risk Reduction. Accessed September 25, 2024. https://www.undrr.org/event/online-workshop-resilience-local-governments-multi-sectoral-approach-integrate-public-health
- UNDRR. Disaster Resilience Scorecard for Cities: Addendum for Education System Resilience for Extreme Weather Events. United Nations Office for Disaster Risk Reduction. Accessed November 26, 2025. https://mcr2030.undrr.org/education-system-extreme-weather-scorecard
- Ryan B, Telford T, Brickhouse M, et al. Strengthening food systems resilience before, during and after disasters and other crises Journal of Homeland Security and Emergency Management 2023;doi:https://doi.org/10.1515/jhsem-2022-0028
- Xiao L, Tian N, da Silva D, Scarazzato L, Karim Z, Ricard J. Trends in World Military Expenditure, 2024. Stockholm International Peace Research Institute. 2025;doi:https://doi.org/10.55163/AVEC8366
- Giordano J. Biotechnology in the FY 2026 NDAA: Strategic Implications — and Recommendations — for Joint Force Readiness. Strategic Insights. Accessed December 18, 2025. https://inss.ndu.edu/news/Article/4358679/biotechnology-in-the-fy-2026-ndaa-strategic-implications-and-recommendations-fo/
- Australian Government. United States Force Posture Initiatives. Accessed March 5, 2026. https://www.defence.gov.au/defence-activities/programs-initiatives/united-states-force-posture-initiatives
- Defense Do. Pacific Deterrence Initiative – Department of Defense Budget Fiscal Year (FY) 2026. Accessed March 5, 2026. https://www.scribd.com/document/933891564/FY2026-Pacific-Deterrence-Initiative
Published: March 27, 2026
Category: Perspectives
Volume: 27 - 2026



